Ethically Diverse Faith Perspectives On Death Literacy and End-of-Life Care



Project leads Dr. Marianne Rozario (left) and Professor Maggie Doherty (right)
Authors: Dr Marianne Rozario, Associate Professor Maggie Doherty from the Centre for the Art of Living and Dying Well - St Mary's University, Professor Sara Spear, Professor Karen Sanders, Professor Jacob Phillips also from St Mary’s University; a Community Advisory Group (CAG) of 4 community members: Simon Romer, Shobha Sharma, Shahin Akhtar, and Suni Patel; the Birmingham Diocese Interreligious Commission, Lancaster University Medical School and the Royal Marsden; Pat Whitney from the Birmingham Diocese Interreligious Commission, Dr Amy Gadoud from Lancaster University Medical School and Dr Joanne Droney from the Royal Marsden.


Sandwell Council staff involved in the project: Suni Patel (left) & Shahin Akhtar (right)
Quick Summary
This study explores how people from different ethnic and faith backgrounds in Birmingham experience end-of-life care, and how understanding of death and dying (“death literacy”) can be improved. The study involved a Community Advisory Group and focus groups with people from Muslim, Hindu, Sikh, Buddhist and Jewish communities.
People from ethnically diverse faith communities in Birmingham have clear religious and cultural needs around dying, death and bereavement. Many of these needs are not currently well supported in hospitals. Improving communication, building mutual understanding, and increasing death literacy—both within communities and among healthcare staff—would help ensure that everyone receives end-of-life care that respects their beliefs, traditions and values.
Objectives
The pilot study aimed to understand how ethnically diverse faith communities in Birmingham experience end-of-life care and how death literacy can be improved. Its main objectives were to:
- Co-produce knowledge on culturally appropriate ways of discussing death and dying within these communities.
- Identify faith-specific barriers and enablers that affect end-of-life conversations and the recording of care preferences.
- Develop recommendations to support more culturally sensitive and inclusive end-of-life care, helping healthcare providers and communities work better together.
Why is this research important?
Birmingham has large and diverse faith communities, yet many people from these groups do not use hospice or end-of-life care services as much as others. National reports also show continuing inequalities in care for minority ethnic groups. The study wanted to:
- Understand what religious and cultural practices matter at the end of life.
- Identify problems people face in hospitals when trying to follow these practices.
- Suggest ways healthcare services and faith communities can work together to improve care.
What we did, with who and how
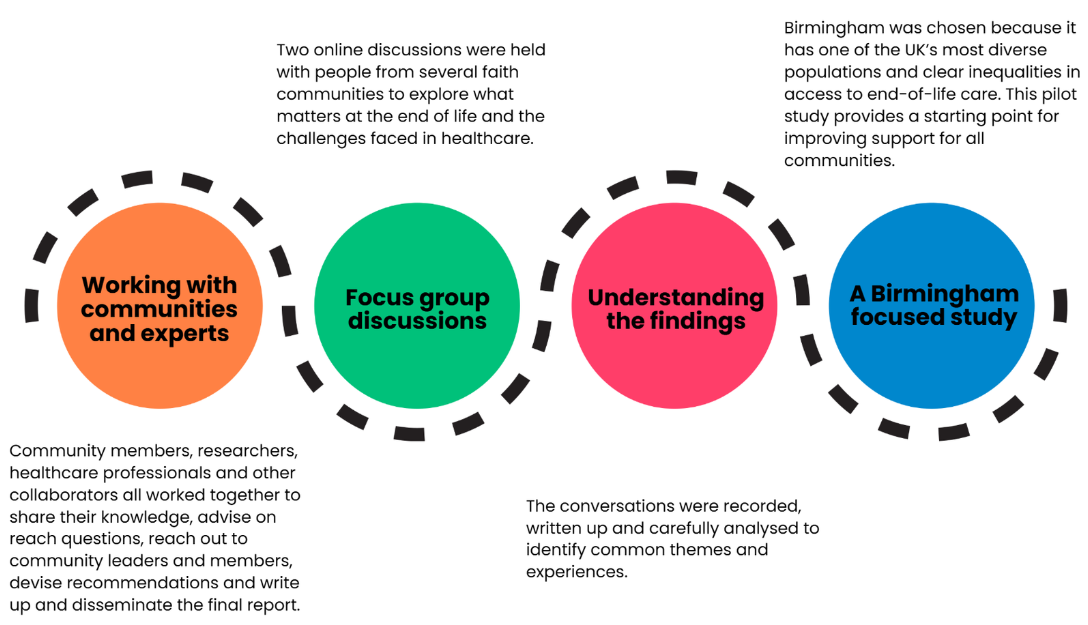
Graphic describing the methods
Findings
1. Important religious and cultural practices at the end of life
Across all faith groups, several practices were described as essential:
Sacred texts, prayers and meditation
People often want sacred verses read to them as they are dying—such as the Qur’an, Bhagavad Gita, Sikh prayers, or Jewish prayers. Buddhists highlighted meditation as preparation for facing pain, fear and death.
Holy water
Muslim participants described the use of Zamzam water; Hindu participants referred to water from the River Ganges. It may be given as a sip or placed on the lips if the patient cannot swallow.
Positioning of the body
Some faiths require the body to be positioned in a certain direction, for example facing Mecca in Islam. Hindus may wish the person to be laid close to the floor.
Post-death rituals
Many communities prefer fast burial or cremation, sometimes on the same day.
- Muslim, Hindu and Jewish traditions often emphasise very quick burial.
- Sikhs usually prefer cremation with specific prayers.
- Buddhists prefer the body to be left undisturbed for longer to allow for peace.
2. Challenges within healthcare settings
Difficulties carrying out prayers or rituals
Hospital wards can be noisy and lack privacy, making it hard to pray or perform rituals respectfully. Some religious items (such as Sikh “5Ks”) may be misunderstood or handled insensitively.
Lack of quiet spaces for families
Families often have nowhere private to gather, grieve or pray together. Multi-faith rooms may not meet the needs of different traditions.
Issues with care of the body
There were concerns about:
- Delays in issuing death certificates and releasing the body, which disrupts traditions requiring fast funerals.
- Bodies being handled in ways not permitted by certain faiths (e.g., for Jews, non-Jewish staff touching the body).
- Autopsies, which are discouraged in some religions but sometimes carried out unnecessarily due to lack of awareness of alternatives such as non-invasive scans.
3. Talking about death and end-of-life preferences
Positive examples
Some communities run workshops on death rituals, body washing and shrouding, and have “death committees” to help families manage funeral arrangements. Some families openly discuss organ donation and care preferences.
Barriers
However, death can still be a taboo topic. People may feel awkward or avoid discussing:
- Their own end-of-life wishes
- Traumatic or “unnatural” deaths (suicide, drug-related deaths, infant deaths)
- Grief and mental health following bereavement
There is also often limited understanding of grief in families and religious communities.
Recommendations

Recommendations to support more culturally sensitive and inclusive end-of-life care
Skills development
Through involvement in this study, Sandwell Council would have strengthened:
- Community engagement skills – working collaboratively with diverse faith groups and building trust.
- Qualitative research abilities – facilitating sensitive conversations, running focus groups and analysing thematic data.
- Cultural and religious literacy – gaining deeper understanding of end-of-life practices across Muslim, Hindu, Sikh, Buddhist and Jewish communities.
- Cross-sector partnership working – coordinating with healthcare providers, faith leaders and academic partners.
- Communication skills – presenting findings clearly, addressing taboo topics, and producing accessible materials for varied audiences.
Benefits for Sandwell
The research findings offer several practical advantages, helping Sandwell Council to:
- Reduce health inequalities by improving access to culturally sensitive end-of-life and bereavement services.
- Strengthen relationships with ethnically diverse communities through co-production and ongoing dialogue.
- Improve public health planning, ensuring commissioned services understand and meet religious needs such as rapid burial or prayer space.
- Support workforce development by informing training on cultural competence and death literacy.
- Enhance bereavement and registration processes, reducing delays that disproportionately affect certain faith groups.
- Advance Compassionate Communities work, enabling more community-led support around death, dying and grief.
To learn more or access this study in another language please contact:
marianne.rozario@stmarys.ac.uk or maggie.doherty@stmarys.ac.uk
Or visit:
https://www.stmarys.ac.uk/research/centres/the-art-of-dying-well/index.aspx